Is the thermic effect of food higher if you are lean?
By Fredrik Tonstad Vårvik
The thermic effect of food (TEF) is the increase in energy expenditure in response to the digestion, absorption and storage of food (1,2). In this article, I explore whether or not the thermic effect of food is higher in leaner individuals.

The thermic effect of food: the research
Protein is the macronutrient that increases your metabolism the most. True. Protein has a thermic effect of 20-30%, whereas carbs are at 5-15% and fat is at 3-4% (3,4). Since meals rarely contain only one macronutrient, mixed meals are often given a TEF of around 10% (1,2).
If two subjects – one having a normal and the other having a subnormal thermogenic response to a meal – increase their food intake, the former will not put on as much weight as the latter (5). Some studies show differences between obese and lean subjects. Most of the research indicates that lean individuals have a higher TEF than obese individuals, both for mixed meals (5–12), and for fat (5), while other studies have found no difference (13–15).
A review by Jonge and Bray in 1997 included 49 studies. About 60% of the studies found a higher TEF in lean subjects compared to obese subjects (16). A newer review by Granata and Brandon from 2002 came to almost the same conclusions: out of 50 studies, 60% found a higher TEF in lean subjects compared to obese subjects (1).
Tataranni et al, who conducted a study in a respiratory chamber concluded that body weight has no association with TEF (2). Worth mentioning here is that the mean fat percentage for the subjects was about 30%±10 for male and above 40%±10 for female, which means there were very few lean (if any?) subjects participating in the study. However, Tataranni et al associates insulin resistance with lower TEF, which has a stronger association with obesity in the literature. This table from Swaminathan 1985 shows the TEF of a mixed meal between the different macronutrients between obese and lean individuals (5). In this study, as we can see, a mixed meal in lean subjects is high, actually higher than the TEF of protein alone, 25% vs 22.5%, respectively.

Numbers up to 30-35% TEF have been reported for protein (4,17). However, since carbs and fat are needed in addition to protein, we most often eat a mixed meal. Therefore, it appears that if you are lean, you can’t get much benefit from increasing your protein, if it is sufficient in the first place.
Let’s take a look at Antonio et al’s two recent studies, where the very high-protein groups had 3.4g/kg/d and 4.4g/kg/d (18,19). In these two studies, there was no difference in improvements in body composition in the 4.4g/kg/d group vs low-protein group, and there were small improvements in body composition in the 3.4g/kg/d group compared to the low-protein group. More precisely, fat percentage decreased by 1.8% more in the 3.4g/kg/d group compared to the low-protein group. This can be explained by a higher adherence to training compared to the lower-protein group, a higher NEAT from the high-protein group (20), or over/under-reporting from dietary recall. Another important point; in the 4.4g/kg/d study, the dropout was high and some of the subjects stated that it was too difficult to consume the high-protein diet. In the 3.4g/kg/d study there was also a higher dropout in the high-protein group, however, the dropout in both studies can be partially explained by a higher number of participants in the high-protein groups. That said, the researchers divided the participants in two unequal groups to take into account the loss of subjects from potential lack of compliance in the high-protein group. So, why follow a diet that you can’t adhere to in the first place anyway? Protein and satiety will be an article for later.
Protein intake in bodybuilders has been noted up to 4.3g/kg (21) however, it is doubtful whether they gained any benefits from it. It may have even been counterproductive, due to the decrease in both fat and carbs, which can have an impact on hormones, vitamins, performance, recovery, etc. If you are obese it may seem like a good idea to follow a diet with a relatively high-protein intake, since the mixed meal in this study only had a TEF of 10%, vs protein of 18.7%.
Why are there conflicting studies?
As we can see, the studies appear to be conflicting, but why is this so? First, methodological factors such as meal size and composition, palatability and timing, measurements <3 hours, short duration, measurement and equipment, environmental factors, and heterogeneity in human obesity may explain different findings (1,2,9). Granata and Brandon mention that in both Jonge and Bray’s review as well as their own, most of the studies with measurements <3 hours reported that TEF was lower in obese individuals, while the minority of studies with measurements >3 hours reported lower TEF in obese individuals (1).
Most studies use variable caloric loads that are dosed after bodyweight or fat-free-mass (FFM), while some use the same caloric load for all subjects. There are problem with both, however, which makes it difficult to compare and conclude. The magnitude of the TEF is strongly related to the size of the caloric load. Thus, when meal sizes are dosed relative to bodyweight or FFM, obese subjects receive larger meals which may bias the comparison to the lean subject. On the other hand, if both receive a given quantity of nutrients, TEF may increase less in obese subjects because their rest metabolic rate (RMR) is higher (15). However, this was not the case when both lean and obese subjects were eating meals with 35% of their RMR (9). Jonge and Bray’s review speculates that factors such as BMI were used and not body fat percentages, that some studies didn’t leave a large enough gap between the upper limit of the lean group and the lower limit of the obese group (16). This could lead to an overlap in the percentage of body fat and thus misclassification between the two groups, which again could lower the chance of finding a potential effect of TEF in different body fat sizes.
If obese people have a lower thermic effect of food, why?
Recent studies suggest that blunted TEF in obese people is related to impaired glucose tolerance and insulin resistance(9,16). From Jonge and Bray’s review, the greater the degree of insulin resistance and body fat, the lower TEF. The same researchers also speculate that lower sympathetic nervous system and higher age could be part of it. Granata and Brandon seem to agree that higher age reduces TEF but believe the sympathetic nervous system theory is more speculative (1). A reduced rate of non-oxidative glucose storage is believed to play a role, which has greater energy cost than glucose oxidation (9). Other explanations that are mentioned are a reduced thermogenesis in brown adipose tissue and skeletal muscle. Tateranni et al also mention lower spontaneous physical activity among the people with lower TEF (2). Another suggestion is that obese people may have reduced sensitivity to the actions of thermogenic hormones that are stimulated with a meal. One reason for this can be because of a sedentary lifestyle (22), as shown in the figure.
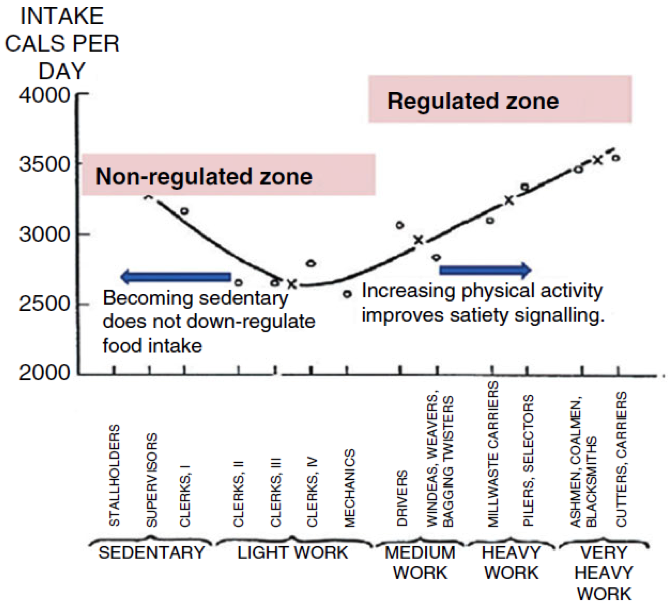
As you can see in the figure, if you are sedentary, you don’t have as good of satiety signaling as if you are active. Regarding the insulin resistance, it has been shown that a reduction in insulin sensitivity down regulates nervous system activity in the postprandial phase, and reduces energy expenditure (23).
If supposed lower TEF in obese individuals is true, the researchers don’t seem to agree if it is part of a consequence of obesity or if it contributes to obesity (1).
Practical applications:
- If you are lean, you may have a TEF of up to 25% for a mixed meal, based on one study. However, since the research is far from clear – you should opt for 10-25% in your calculations, as the research slightly favors a higher TEF in lean subjects. So maybe, just maybe, you can enjoy an extra scoop of ice cream without bad conscience if you are lean.
- If you are obese, you should remain on the safe side and assume you have a lower TEF than lean individuals. Opt for a TEF up to 10%.
From the data available, it is clear that we need much more controlled research in this area.
References
- Granata GP, Brandon LJ. The thermic effect of food and obesity: discrepant results and methodological variations. Nutr Rev. 2002 Aug;60(8):223–33.
- Tataranni PA, Larson DE, Snitker S, Ravussin E. Thermic effect of food in humans: methods and results from use of a respiratory chamber. Am J Clin Nutr. 1995 May 1;61(5):1013–9.
- Jéquier E. Pathways to obesity. Int J Obes Relat Metab Disord J Int Assoc Study Obes [Internet]. 2002 Sep;26 Suppl 2. Available from: http://dx.doi.org/10.1038/sj.ijo.0802123
- Halton TL, Hu FB. The effects of high protein diets on thermogenesis, satiety and weight loss: a critical review. J Am Coll Nutr. 2004 Oct;23(5):373–85.
- R Swaminathan RFK. Thermic effect of feeding carbohydrate, fat, protein and mixed meal in lean and obese subjects. Am J Clin Nutr. 1985;42(2):177–81.
- Tappy L. Thermic effect of food and sympathetic nervous system activity in humans. Reprod Nutr Dev. 1996;36(4):391–7.
- Dabbech M, Boulier A, Apfelbaum M, Aubert R. Thermic effect of meal and fat mass in lean and obese men. Nutr Res. 1996 Jul 1;16(7):1133–41.
- Schutz Y, Bessard T, Jéquier E. Diet-induced thermogenesis measured over a whole day in obese and nonobese women. Am J Clin Nutr. 1984 Sep;40(3):542–52.
- Segal KR, Edaño A, Blando L, Pi-Sunyer FX. Comparison of thermic effects of constant and relative caloric loads in lean and obese men. Am J Clin Nutr. 1990 Jan;51(1):14–21.
- Segal KR, Edaño A, Tomas MB. Thermic effect of a meal over 3 and 6 hours in lean and obese men. Metabolism. 1990 Sep;39(9):985–92.
- Segal KR, Gutin B, Nyman AM, Pi-Sunyer FX. Thermic effect of food at rest, during exercise, and after exercise in lean and obese men of similar body weight. J Clin Invest. 1985 Sep;76(3):1107–12.
- Segal KR, Gutin B, Albu J, Pi-Sunyer FX. Thermic effects of food and exercise in lean and obese men of similar lean body mass. Am J Physiol. 1987 Jan;252(1 Pt 1):E110–7.
- Blundell JE, Cooling J, King NA. Differences in postprandial responses to fat and carbohydrate loads in habitual high and low fat consumers (phenotypes). Br J Nutr. 2002 Aug;88(2):125–32.
- Segal KR, Gutin B. Thermic effects of food and exercise in lean and obese women. Metabolism. 1983 Jun;32(6):581–9.
- D’Alessio DA, Kavle EC, Mozzoli MA, Smalley KJ, Polansky M, Kendrick ZV, et al. Thermic effect of food in lean and obese men. J Clin Invest. 1988 Jun;81(6):1781–9.
- de Jonge L, Bray GA. The thermic effect of food and obesity: a critical review. Obes Res. 1997 Nov;5(6):622–31.
- Binns A, Gray M, Di Brezzo R. Thermic effect of food, exercise, and total energy expenditure in active females. J Sci Med Sport Sports Med Aust. 2015 Mar;18(2):204–8.
- Antonio J, Ellerbroek A, Silver T, Orris S, Scheiner M, Gonzalez A, et al. A high protein diet (3.4 g/kg/d) combined with a heavy resistance training program improves body composition in healthy trained men and women – a follow-up investigation. J Int Soc Sports Nutr. 2015 Oct 20;12(1):39.
- Antonio J, Peacock CA, Ellerbroek A, Fromhoff B, Silver T. The effects of consuming a high protein diet (4.4 g/kg/d) on body composition in resistance-trained individuals. J Int Soc Sports Nutr. 2014 May 12;11(1):19.
- Bray GA, Smith SR, de Jonge L, Xie H, Rood J, Martin CK, et al. Effect of dietary protein content on weight gain, energy expenditure, and body composition during overeating: a randomized controlled trial. JAMA J Am Med Assoc. 2012 Jan 4;307(1):47–55.
- Spendlove J, Mitchell L, Gifford J, Hackett D, Slater G, Cobley S, et al. Dietary Intake of Competitive Bodybuilders. Sports Med Auckl NZ. 2015 Apr 30;
- Blundell JE, Gibbons C, Caudwell P, Finlayson G, Hopkins M. Appetite control and energy balance: impact of exercise. Obes Rev Off J Int Assoc Study Obes. 2015 Feb;16 Suppl 1:67–76.
- Watanabe T, Nomura M, Nakayasu K, Kawano T, Ito S, Nakaya Y. Relationships between thermic effect of food, insulin resistance and autonomic nervous activity. J Med Investig JMI. 2006 Feb;53(1-2):153–8.
About the author

Fredrik Tonstad Vårvik is a personal trainer & nutritionist. He writes articles and work with online coaching at FredFitology. Follow him and his colleagues at Facebook & Twitter. Check out FredFitology for more info.




So are fat people fat because they have lower TEF or do they have a lower TEF because they are fat?
They are most likely having a lower TEF because they are fat.
So basically, it’s easier to stay lean if you’re already lean than it is to actually get lean?
(Damn, that’s a lot of “leans” for one sentence…)
Good article, Fredrik! Thanks for summing up the literature on this topic.
I am wondering if there is a slight mistake with the wording here:
“most of the studies with measurements 3 hours reported lower TEF in obese individuals (1).”
It seems you are saying TEF is lower in obese individuals regardless of measurement time differences, but the sentence above seems to say that this measurement timing should make a difference.
I know this is a very minor point, but just wanted to make you aware of it.
Thanks again!
Hey Zach and sorry for the late reply!
Glad you liked the article. Yeah the authors stated that measurement time could have something to say, along with the other reasons I mentioned. Overall it seems like there could be a minor difference, based on my interpretation of the research.