Today I have a guest-post for you by Dr. Conrad Stalheim, a CSCS and chiropractor out of Iowa (see his bio below). This is a great article!
Anterior Pelvic Tilt and Lumbosacral Pain as it Relates to the Hip Thrust and Glute Bridge – by Conrad Stalheim
Bret has gone to great lengths to discuss how to properly perform the hip thrust and glute bridge and some common mistakes that can lead to pain and injury. He has also been very clear that this exercise needs to be progressed intelligently like any other exercise.
If you are like me, the only problem is that he has a ton of posts and videos, so I tend to jump to the ones with the 120lb women bangin’ out reps at 250#’s and above and then think that I should go heavy to start.
It never hurts to revisit the basics or gain another intelligent perspective.
This post will address:
- The biomechanical fault of lumbosacral hyperextension.
- How that fault predisposes you for pain and injury.
- How that fault manifests in the glute bridge/hip thrust, deadlift, and various other movements.
- How I cue and progress individuals in a clinical setting to gain the motor control to activate the glutes and spare the spine.
Remember, the glute bridge is performed with your back on the floor, and the hip thrust is performed with your back elevated.

The Hip Thruster is the best way to do the hip thrust – stable and versatile!
When I first started loading these “heavy”, I hurt myself in what I think is probably the most common injury with this movement.
LUMBOSACRAL HYPEREXTENSION
Extension hypermobility at the lumbosacral joint (L5-S1) is very common. This is one of the joint regions that we commonly see excess motion, which is why it is one of the most common sites of degeneration. When muscles don’t provide the necessary stability, your body will create it another way.
These are some strong indicators that you are prone to or living in a state of lumbosacral over-extension:
- Significant Anterior Pelvic tilt
- Tight Hip Flexors
- Lack of global extension and more of a hinge in one particular spot
- Weak abdominal musculature – I find it more difficult to evaluate this one, but it is also likely present, and it doesn’t hurt to address it.
aka Lower Crossed Syndrome
I’m actually glad that I hurt myself, as it exposed me for not taking care of a dysfunction that I’ve known about but just didn’t have the motivation to take care of. This isn’t just a hip thrust issue. This faulty movement strategy is going to show up in deadlifts, pull-ups, overhead presses, etc. Watch the video further down if you want to see the same movement fault applied to the deadlift.
I’m not going to go into loading and progressing hip thrusts and glute bridges. As a clinician, I’m generally working with people who are in pain so I’m not throwing a barbell on their hips. I’m all for loading these exercises, and I do so myself, but my particular skill set and objectives with patients is for rehab. Something I have to teach in nearly every case is proper pelvic tilt, spine position, bracing, and motor control to activate the glutes, NOT all the other various compensatory muscles that people activate instead of their glutes.
So back to the issue of lumbosacral hyperextension…
We generally think of mobility as a good thing. The more flexible a person is the better, right?
In the book Movement Impairment Syndromes, Shirley Sahrman writes, “When a system is multisegmented, as in the case of the human movement system, the greatest degree of motion occurs at the most flexible segment. This follows the laws of physics, which states that movement takes place along the path of least resistance. Thus most spine dysfunctions occur because of excessive relative flexibility, particularly at specific segments, rather than at segments of reduced flexibility. The reduced flexibility of some segments invariably contributes to compensatory motion at the most flexible segments.”(1)
Essentially, we would like to see all joints contribute and participate in their role in movement. We do not want to see one joint stand out as the place of excess movement.
Here’s an impressive global extension curve vs a lumbo-sacral hinge.

Clearly the woman in the photo on the left has a substantial amount of hinge at the lumbosacral joint, but she also shows a good example of a uniform extension curve through the spine.
Below is another example. Again we can see more of a uniform extension curve on the left vs. a more straight thoracic spine and greater lumbosacral extension hinge on the right.
This isn’t the best angle but good enough to get the point. The woman on the right actually appears to have pretty decent global extension compared to many but also has enough of a “hinge” to see the difference.
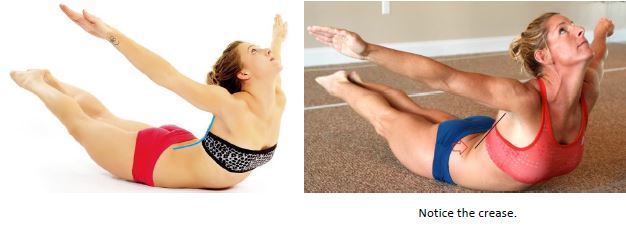
Although everyone needs to stabilize their lumbar spine to get the most out of hip thrusts and glute bridges, you are much less likely to get injured if you don’t have a hypermobile segment, as you will spread the forces out over more segments.

Above you can see some lumbar arching/extension in both pictures, but in the first one, the woman’s ribs are starting to flare upwards and towards her head indicating that she is not stabilized in her spine.The picture on the right shows potentially a little more lumbar extension than we would like to see, but she appears to have her abs engaged and ribs locked down. You can see that her hips haven’t fully opened/extended but she is likely at her hip flexor end-range, and additional extension would probably come from her lumbar spine.
So why don’t we all just inherently adopt a better pelvic position and do this movement correctly?
In a sense, it’s because we’re lazy, not necessarily on purpose but because we don’t know any better.
We tend to adopt positions that allow us to “HANG” on our tissues. We inherently search for stable positions, but creating stability muscularly is more metabolically expensive, so we hang on the “passive” structures like ligaments and joint end-range.
We do this in long-duration, low-load activities like standing and sitting, but we also do this when weight gets too heavy, and our muscles can’t support it.
Our passive tissues can handle this up to a point, and it works to accomplish the task or APPEARANCE of a full movement, but the price can often be pain and injury.
For a little extra credit, you can check out this video of Kelly Starrett showing this same over-extended pattern with the deadlift. You can learn every movement and exercise individually, or you can learn the concepts, allowing you to self-correct and take care of yourself or your clients.
ADDRESS YOUR TIGHT HIP FLEXORS
If tight hip flexors are an issue for you, you will have to address it in order to really achieve full range of motion on the Hip Thrust. If you don’t, you will either have to stop short of full hip extension range, or you will have to use lumbar hyperextension to make it look like (and make yourself feel like) you are getting full range of motion.
Here’s one way to test for tight hip flexors:
Lying on a table or bench, pull one knee tight to your chest, and let your other leg hang. The hanging leg should easily fall to parallel with the floor.
Keep your lumbar spine flat
(e.g. you shouldn’t be able to slide your hand under your low back.)
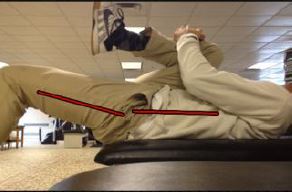
Here’s how we address those tight hip flexors:
It’s called the couch stretch, so you don’t have an excuse not to do it. You can literally do it on your couch while you watch tv. Hang out on each side for at least a few minutes every day for a week and see what happens.

Don’t cheat by using lumbar extension like the picture on the right.
This isn’t the only way to accomplish this stretch, but it gives you the basic idea on “opening” the hip up into extension.
After the stretch, I always think it’s a good idea to use that slight increased mobility, and fill it in with some stability work. This should program your brain that you can handle this increased mobility. I’d hit 1-2 sets of 10-15 bodyweight hip thrusts or glute bridges with an emphasis on really squeezing your glutes to get a couple of extra degrees of HIP extension NOT LUMBAR extension.
Groove the Motor Pattern to SPARE your back and better ACTIVATE your glutes.
Since I have a limited amount of time to work with people in pain who are not always the most athletic, I always try to find the most simple and quickest fool-proof cues. But don’t worry, there’s always somebody who will find a way to mess up even the best cues.
As a quick, somewhat related digression, here’s how I generally fit glute strengthening into patient rehab.
Evidence suggests to us as physical medicine practitioners that joint manipulation works quite well for acute episodes of low back pain, as in pain that’s only been around for a few weeks. It doesn’t tend to work as well for chronic cases of back pain such as those who have had pain for months, years, or regularly recurring episodes. (2)
For chronic cases, I have found good success using a manual therapy approach for pain control to start. These are things like joint manipulation, myofascial work, flexion-distraction, and a multitude of other techniques to reduce pain, inflammation, and break the pain cycle. Along with manual therapy, I think it is crucial to address and reduce specific exacerbating factors by teaching general spine/tissue sparing strategies. It generally doesn’t take long for most patients to be able to start working on core bracing and stability techniques. Stu McGill has given us a great resource in his book Low Back Disorders (3) for how to spare the tissues and utilize intelligent progressions of static and dynamic core stability exercises.
Once we’ve learned how to move properly to spare our tissues and create a stable and neutralish lumbar spine, we still need a way to pick things up, move a heavy load, and project ourselves through space. This applies whether you’re an athlete or not. This is where I think Bret is providing a unique and great resource, from primitive glute activation patterns to more advanced, heavy, glute loading exercises.
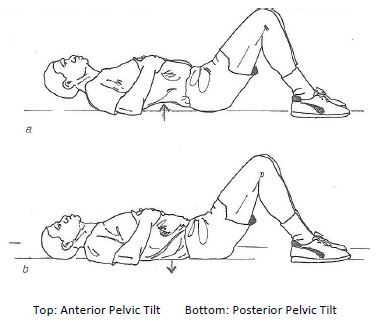
Clinically, I like to initially teach this movement pattern with your back flat on the ground and making sure you can anteriorly and posteriorly tilt your pelvis. To begin the movement, you want to posteriorly tilt your pelvis and press your lumbar spine flat to the ground. You should feel your abs and core musculature get stiff. Maintain that position as you drive your heels through the ground and lift your trunk off the ground by contracting your glutes.
I personally like to start with my heels fairly close to my butt as I feel that this facilitates more glute and less hamstring activation.
Again, if your hip flexors are tight, then you can’t and shouldn’t go for full hip extension – you won’t get it. But you should work on it, as it’s going to limit glute activation (reciprocal inhibition).(4) You also need this full hip-extension for a functional running stride, golf swing, kettlebell swing, and to be able to move and perform optimally in general.
If this is still a struggle, here’s a trick that makes it almost impossible to hyperextend your lumbar spine. Pull one knee into your chest. I would personally start with my heel closer to my butt than the picture below illustrates. The ball in the hip crease is good for those with a tendency to cheat, but it’s not necessary.

Taking the time to develop the correct motor program with adequate mobility should allow you to progress this exercise safely with better ability to engage your GLUTES and self-regulate for injury prevention.
Remember:
- Gain the motor control/technique to feel these without weight before loading.
- Bret has emphasized the need to find the right height bench for hip thrusts – this is important
- Don’t use a weight or continue a set that you are unable to maintain the posterior pelvic tilt position with.
BIO:
Conrad Stalheim, DC, CSCS, SFMA, is the owner of Iowa Chiropractic and Performance Center. In addition to using manual therapy, he incorporates assessment and treatment of dysfunctional movement patterns leading to pain and injury. He has found it important clinically to increase glute activation and strength, especially in cases of low back pain.
Sources:
- McGill, Stuart. Low Back Disorders: Evidence-based Prevention and Rehabilitation. Champaign, IL: Human Kinetics, 2007. Print.
- Sahrman, Shirley. Diagnosis and Treatment of Movement Impairment Syndromes. St. Louis: Mosby, 2002. Print.
- Knierim, James, PhD. “Spinal Reflexes and Descending Motor Pathways.” Spinal Reflexes and Descending Motor Pathways.” Department of Neurobiology and Anatomy – The University of Texas Medical School at Houston, Web. 03 Apr. 2013.
- Childs JD, Fritz JM, Flynn TW, et al. A clinical prediction rule to identify patients with low back pain most likely to benefit from spinal manipulation: a validation study. Ann Intern Med 2004;141(12):920–8.




This article is indeed a keeper. Thanks for sharing!
Interesting article, Bret, although I have the opposite problem to hyperextension / hypermobility as I have lumbosacral fusion (together with degenerative discs and muscle spasm), with significantly impaired range of motion in this area…I can do glute bridges with no problem but doing the hip thrust even without weight causes some pain in my lower back 🙁
I have 15 levels fused and I am attepnting to improve my butt area. Any tips ? Which exercises had worked for you ? I can easily do both with weight but I get musle spasms of my spine stabilizators on just one side of the fusion.
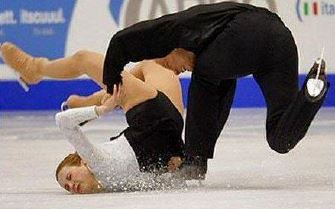
Great article, and a great resource for my work with figure skaters and their lower back issues – thanks!
I feel like I have found some commonalities across a bunch of different stuff I have been reading to “fix” lower crossed syndrome.
1. Soft tissue work on hip flexors, adductors
2. Mobility and stretching of hip flexors and adductors
3. Glute/hamstring activation and strengthening
4. Creating appropriate core stability
I also have been reading recently that breathing patterns play a large role in many postural issues, and although I do not know very much about them, I was thinking that Gray Cook’s crocodile breathing drill seems like a pretty good bang for your buck.
Do you feel that lower crossed syndrome is more of a motor control issue or a strength issue, or both? I am still trying to fix it on myself, and I am thinking that the two are very related, but I am not sure. On one hand, Gray Cook tells us not to get caught up in strengthening things, and that we should focus on the fundamental stability, mobility, and movement patterns. On the other hand, Robertson and Cressey take more of an approach of soft tissue work and mobilization of the short tissues, and strengthening the lengthened tissues. How does one find the underlying principles for these seemingly different approaches?
Very good question. Addressing this could be its own post. I’ll keep it as short as I can.
I think that most issues, including Lower Crossed Syndrome have an element of mobility, stability, AND Motor Control. So I can’t say which is more important as they’re all significant.
I love the content Gray Cook puts out and learning from him. I believe that Cook contends that we should not load strength on dysfunction – that we gain mastery of fundamental stability, mobility and movement patterns BEFORE strengthening. I think he can make it SEEM (at times) like there are sort of “magical” fixes to issues, at least to me. Like there is a simple way to restore proper movement patterns on a sub-conscious level, which once “fixed” you won’t have to think about again. I’m not saying that this is what he thinks or says and I’m not saying this doesn’t happen. There are definitely ways to quickly and automatically fix a motor control issue (e.g., running with nice padded shoes and jamming your heels into the ground on each stride – take the shoes off and your gait SHOULD change naturally unless you ignore pain signals from your heels.) I think that much of motor control especially in the beginning and sometimes FOREVER, is a CONSCIOUS process. I have to decide if I’m going to activate the proper muscles to stand or sit with optimal posture, brace my core before I stand up, hip hinge when I bend over, let my knees cave when I squat, etc.
My experience, and I believe theory and research would support it, is that tissue takes time to remodel and adapt to demands place on it. If you sit a lot in a position where your hip flexors are shortened, it’s going to take some good concerted effort and time to remodel and undue that shortness. Mobility issues tend to take much longer to correct than stability/motor control issues.
That was a great article. However I had to read it about three times. Prior to reading the article I was actually trying to have some arch in my lumbar spine when I did the exercises.
If you already have a video addressing this issue repost or direct us to it.
Thanks for your kind comment! Imagine what it was like before I chiseled it down…
Bret may have more to add to this but as you requested and for those who are video inclined:
http://www.youtube.com/watch?v=h5WhWu1g080 (From about 8:00-9:30 Bret has specific spinal model demonstration for the hip thrust)
http://bretcontreras.com/everything-you-need-to-know-about-the-hip-thrust/
(As the title suggests – video demonstration on what you need to know)
Loved the article. I now notice that a lot of “online” trainers with programs they sell that would have us do these type of exercises don’t emphasize correct stance from the beginning. They are too quick in getting us to simply do the exercise so we can proceed to the next one. It’s so helpful seeing demonstrations like this with lots of visuals.
Bret, you are simply a fantastic source of good training methodology. Love “Strong Curves”!
Bret, sometimes i find that some of your guest posts are not in the class of your own posts. This is different and a truely fantastic post. Great complement to your own work. I have a question for you or conrad, can the hip thrust strain the hamstrings? If so, what is the correct form to prevent that? Thanks for the great post.
Very much appreciate the compliment!
The Hip Thrust could certainly strain the hamstrings. A couple things:
1. I like to start with the Glute Bridge so that when you tilt your pelvis posteriorly you can feel the feedback of your lumbar spine flattening to the ground.
2. I bias my feet closer to my butt rather than further away.
3. Some people put their toes against a wall and as they drive up they push their toes into the wall to activate their quads for the reciprocal inhibition effect to the hamstrings. I prefer to drive my heels down and away through the ground (maybe a 45 Deg. angle down and away) to create the same effect.
4. Concentrate on maintaining the post. tilt the whole way up (your abs should be stiff and engaged) and really squeeze the post. tilt at the top.
5. Take all this to the Hip Thrust. It’s possible that a person may do better starting with the Hip Thrust, I just find it easier to control and cue the Glute Bridge for instructional purposes.
Since it’s very common for the hamstrings to be a bit dominant over the glutes, I find it helpful to instruct people to use their fists and push up on their glutes to give themselves a little help. It enhances the mind-muscle connection as you can feel how contracted or not your glutes are and lightens the load so the person feels more in control and isn’t merely trying to SURVIVE the movement.
Phenomenal post. Everything you discussed relates to the direction I’ve taken my own training. Yes, I am one of those distracting ladies in the video hip thrust heavy weights, but I have my limitations and mobility issues to work through as well.
You’ve laid it all out in such a concise manner and this is an important read for all of my clients. Thanks so much!
BTW, the comment at the end of Kelly’s video relating to endurance athletes. I can’t tell you how many times I’ve wanted to pull over and correct these distance runners I see with their knees banging together as they run for miles on end. 🙂
Thanks Kellie!
Nice job on those heavy hip thrusts!
I love watching runners as I drive as well. So many unique gait patterns. Let me know how it goes for you if you ever pull over and give out some instruction!
Conrad was my college roommate. This is awesome.
Well, I should clarify. He lived on my floor…Friley
Conrad – I have had disc herniations (L5-S1 of course) and ended up with significantly weakened glutes due to several years of just avoiding anything that required use of my lower back/hips. Discovered that avoiding use of my back didnt actually mean I avoided re-injury and instead caused other problems (hip flexors, weak glutes etc etc)…anyway, just wanted to say fantastic article covering (for me) the rehab steps and what I need to make sure I have right before progressing. I am the type of guy who will jump to hip thrusting bodyweight…
One question I have (for you or maybe Bret) is that I find my hip thrusts/glute bridges cause muscle soreness in my gluteus medius rather than gluteus maximus. Is this because I’m doing them wrong, or is it a function of having a particularly weak gluteus medius or tight hip flexors etc? Or is it just one of those things
Hey Chris! Thanks!
Hard to say without seeing you do the movement why you would be feeling it more in your glute med. I wouldn’t necessarily think that was a big deal or indicative of doing them wrong. There doesn’t seem to be a large amount of eccentric stress with these movements, so I wouldn’t expect a large amount of glute max. soreness. The glute med. however may be stabilizing pretty hard during the movement. Like sore abs after pull-ups – we often don’t realize how hard the stabilizing muscles work.
I have a similar problem that started with sciatica symptom with numbness. My symptoms have since improved and I am onto the rehab with a focus on glutes.
I find that when contracting into the bridge I get a momentary return of my symptoms which stops the exercise for me. Day to day this prevents me from a full foot stride on that side. Additionally when doing back (pelvis) extensions this pain occurs when doing on the opposite side. Is this just over active piriformis and how should I rehabilitate the muscles around to take over without the pain?
Many thanks,
Lee
Ps love the podcasts- my favourite one being paleo and crossfit.
Conrad
Nice post. I regularly read online article and tie them into my own training regime.
Do you have a blog to follow?
Thanks Randy!
I have a blog at my website: iachiropractic.com
Currently I post about once a month.
I also work in rehab and many of my patients have no idea how to activate their muscles properly. I have a very hard time getting people to understand the proper way to do the posterior pelvic tilt. Do you have any recommendations for cuing this exercise?
I usually demonstrate first and then have them do it.
I like exaggerated movements to start. It helps to have them anterior tilt first so they get the feel for the overall motion and sometimes feeling an exaggeration of an anterior tilt helps them to exaggerate the posterior tilt. Putting your hands on their hips and giving them pressure in the right direction can help. You have to squeeze your glutes in order to posterior tilt – sometimes just telling a person that helps them to get it.
I also have them anterior and posterior tilt laying on their back and putting their hand under their lumbar spine (see pic towards end of article). I have them create a big arch (ant. tilt) and then have them press their lumbar spine flat to the ground and squish their hand (post. tilt). Of course there is no glute activation at this point but they need to be able create a stiff core first (and be able to maintain it during bridge/thrust). If it seems like someone struggles to activate their glutes and posterior tilt as they bridge up, I put my hands on their hips and create pressure in the posterior tilt direction while also lifting and taking some of the weight off. I also have people use their own hands and help themselves by pushing up on the glutes. This serves to take weight off and gives them feedback on the contraction of their glutes. I wrote a comment a few up that has some other stuff on cueing. Hope this helps!
Thanks. I was doing most of this except exaggerating the ant. tilt first. Great idea, I’m going to try it this week.
I have this exact problem and was coming to similar (though less knowledgeable) conclusions. Thank you for explaining it so thoroughly!!! I started off hip thrusting lots of weight, but wasn’t actually using my glutes and ended up with pain, deloaded, figured out stuff about my ribs, breathing, and alignment and am working my way back up. Thanks for providing the details behind what I “knew” but could not explain nearly as well.
Another way I like to make sure I’m not in anterior pelvic tilt is to concentrate on thrusting with the lower glute/upper hamstring area while keeping my spine as stable as possible. I find that it does allow me to reach full hip extension. Also, thanks for introducing me to the couch stretch. I’ll be doing that on my bed every morning and evening from this day on.
One issue I’m curious about is your take on sitting. What is the normal lumbar position when one is sitting at a desk? I’ve heard people say sit up straight and others say it’s okay to hunch a little at times and that staying rigid in one position for too long is detrimental to the spine. I know I’m speaking in layman terms here, but I hope you understand my question.
Great, insightful post!
Yeah it seems that the older advice was to maintain a neutral to somewhat extended lumbar spine for the entirety of sitting. Now we’re saying that the best seated posture is the one that is changing. Since being fidgety isn’t always conducive to getting work done or appropriate, the neutral and supported lumbar posture should be your “go to” posture. Just don’t be afraid to change it up. Ideally a person is getting up and moving around every 15-20 minutes. Spending a little time in a lumbar-flexed seated posture is fine – just don’t hang out there all day and don’t stand up from that position – reorganize before standing up. Lastly, if a person is flexion or extension intolerant or has some other positional pain exacerbation then they need to really limit that position, at least while healing.
footnotes 1& 2 are mixed up- with all the “stuff” to read I started looking at sources so I don’t loose my mind 🙂
Great article…cleared up a lot of my confusion on proper technique, especially for deadlifts, for this relative newbie! However, I do have some lingering confusion regarding executing the glute bridge and hip thrust with a posterior pelvic tilt vs. with a neutral spine. Do you advise a posterior tilt only in the beginning to ensure glute activation and then train with a neutral spine, or is posterior tilt the best form? I always thought neutral spine was ideal for all/most movements. Or is posterior tilt best only for the hip thrust and glute bridge, but not for other glute focused exercises?
Thanks for all the education!
You are correct, neutral spine/pelvis is your go-to position. When you contract your glutes, your pelvis should be pulled in a posterior tilt DIRECTION (based on muscular attachments). It’s not so much that you are going into some exaggerated posterior tilted pelvic position, you’re actually probably only getting to a neutral pelvic/spine position or maybe slight posterior tilt.
Always start the move in a neutral position and end in a neutral position. The cue of posterior tilting is really just to get the core musculature engaged to brace a neutral spine and THINKING posterior tilt to help contract the glutes and get people away from either starting in an anterior tilt position or ending there.
コロンビア フリースジャケット
Great post. Having so many issues with my right hip flexor spasming. Stretching really aggrevates it more. I play roller derby and time off to work on shoulder inflammation. Started gym and had the same flexion issues doing loaded squats as in the video. (Going to try knees out). Its been 7 months, progress is slow. even after months of oesteo treatment and core work. Went back for a skate last night. 10 min in im spasming and can hardly walk. Any advice?
Super comprehensive post!
I specifically struggle with tight hip flexors so will be giving those exercises a try.
Thanks for posting, Bret/Conrad.
Haydo
Hi Bret,
I have recently started adding barbell glute bridges to my work outs. I try to have proper form and do not feel like I’m arching my back but in the morning I wake up with lower back soreness. I have Harrington rods from scoliosis surgery so I’m not sure if that has anything to do with it. Do you have any suggestions?
Thanks!
I have apt & it is very painful, I cant seem to get any relief, I had a pulled ligament for 8 years before a pt found it, he said he also fell off a roof so he knew the sytems, I could barely walk or put pressure on my leg, I only have it on my left side, my right is pretty normal & doesn’t hurt at all, except in my lower back a little, but not in the hip or groin area, is there any excercises I can do with a stretch or resistance band for anterior tilt? Thank You
Reply ↓
this horrible pain is on my left side in the groin area, in the crack of my leg & pelvis, its feels like i got stabbed with a stake or cro bar & its still in there, Hurts so bad, I was diagnosed with apt, the only thing that seems to help just a little is the lunge with leg against wall & that hurts so bad to do, are there any other excercises or stretches I can do with the stretch or resistance bands, I went to the site you gave me & have tried those, I have done a couple excercises with the resistance band but want to make sure im doing the right ones? I don’t want to do the wrong stretches & pull something out of place or make it worse. If you can give me any advice on excercises, stretches for this it would be gratefully appreciated, Its a deep Aching pain 24 hrs a day & its right a the top of my leg on the inside of that bone or ligament,cartlidge, think its a hard piece of ligament or cartlidge, feels like its on the side of that band (whatever it is), I would like to use the resistance bands if you have any excercises I could do with those, I think I would probably get quicker results using them, thanks again
Hi Bret, may I use the image of posterior and anterior pelvic tilt for a blog post. Thanks in advance.
Thanks for the post Bret, This is what I am looking for !
Defiantly the trouble I’ve found even the simplest of flute bridges painful.
As an ex gymnast I seem to be cut off at lumbar.
Hip flexor now tight as he’ll as I find myself sitting most the day.
Now at 32 and a mother of 3 I see my peers so more mobile that me makes me mad.
Signing up for your newsletter for some solace.
Cheers