Considerations for the Rehabilitation of the Post-operative Knee: Restoring the Athlete’s Active Knee Range of Motion
Robert A. Panariello MS, PT, ATC, CSCS
Professional Physical Therapy
Professional Athletic Performance Center
New York, New York
During the course of rehabilitation of the post-operative knee pathology athlete, common interventions utilized in the field of Sports Physical Therapy and Rehabilitation include the use of modalities for pain, edema, and neuromuscular control, restoration of the knee joint range of motion, lower extremity strength, proprioception, and normal gait, as well as structured treatment progressions to the achievement of the eventual milestones of running, jumping, cutting, and additional athletic activities, and “functional tasks”. All of these milestones are achieved through a number of various treatment methods, manual techniques, exercises, and practices.
Specific training techniques may also be implemented in the clinical setting that may be more suitable in preparing the post-operative knee athlete for the eventual goal of sprinting/running. Proper running technique will not only result in the ability of the athlete to return to their pre-injury running velocities, but also prepare the athlete to partake in an off-season performance enhancement training program or the return to in-season sports participation and training. The training techniques described in this article are those that have been imparted upon me or those adapted to the clinical setting based on my experiences as a Head Strength and Conditioning (S&C) Coach.
By instrumenting these exercise techniques during the rehabilitation process, empirically I have found (a) the athlete is better prepared to technically return to optimal running velocities as well as (b) upon their return to performance enhancement training it is not necessary for the S&C Professional to instruct the athlete in these exercise techniques as more valuable time may now be utilized for the enhancement of the athlete’s physical qualities as well as advanced running techniques.
Restoring Active Knee Range of Motion
The concept of restoring full active range of motion (AROM) of the post-surgical knee during the rehabilitation process was instilled upon me approximately 30 years ago by my good friend Dr. Donald Chu. Over the years Dr. Chu, as well as myself, have both lectured and written with regard to this rehabilitation topic. Although there appears to be professional interest in this information, at the conclusion of their rehabilitation many athletes who arrive to our facility to return to their athletic performance enhancement training, still lack the necessary knee AROM for optimal running performance.
AROM of the knee is imperative to achieve the proper positioning of the heel of the foot at (approximately) the level of the gluteal fold during the swing phase of the running gait cycle. The swing phase comprises 30% of the running cycle, thereby it is very important to re-establish proper back side (swing phase) mechanics. Since the sprinting/running gait cycle is truly a “cycle” if one phase of the running cycle is not efficient, the entire cycle becomes inefficient.
The majority of post-operative knee patients achieve full passive knee range of motion (PROM) during their course of rehabilitation. This is important as the compliance of the soft tissue structures must be established for the eventual proper positioning of the heel of the foot during the swing phase/back side mechanics of the running gait cycle. However, during actual running performance this heel position is only achieved by AROM efforts of the knee, and not due to passive motion (Figure 1).

Figure 1: The Heel/foot Position during the Sprinting and Running Gait Cycle
Why is this foot position important in the running gait cycle?
It has already been stated how the sprinting/running gait cycle is a “cycle” and thus if one part of the cycle is inefficient (the swing phase) the total cycle will also become inefficient (the stance phase). One common cue to ensure the proficiency for the transition of athlete’s backside mechanics to front side mechanics is instructing them to “step over the knee”, as the swing leg moves forward to transition to the initial ground contact of the stance phase of the running cycle. The proper positioning of the heel to the buttock assist to ensure that proper backside mechanics will occur to place optimal force into the ground surface area during the brief period of the stance phase of sprinting/running cycle.
Not establishing a proper heel position due to the lack of knee AROM creates a greater lever arm (distance from) the hip musculature as well as establishes a situation that makes it extremely difficult for the athlete to “step over” the knee (Figure 2).

Figure 2: Heel and foot position due to a lack of knee AROM
As a result of this unsuitable foot placement, during the swing phase transition, the foot will likely pass below the opposite knee resulting in greater friction or “braking” at the time of ground contact. In conversations with various track and field sprint coaches, it has been stated that the combination of inefficient back side mechanics resulting in an unproductive total running cycle, as well as the addition of the consequential increased friction (braking) that also occurs, likely results in a one hundredth of a second increase in running time for each leg cycle performed. How does this affect the athlete’s running performance? Let’s assume that a fairly good 40 yard dash will require the athlete to complete the task in approximately 18 strides. If an inefficient running cycle due to a lack of knee AROM exists, and a likely increase of .01 seconds per stride then transpires, then the following scenario is likely to ensue:
18 strides X .01 seconds = up to an additional .18 seconds (slower) for the 40 yard sprint
Poor backside sprinting mechanics likely results in slower sprint times.
How is AROM of the knee achieved during the rehabilitation process?
AROM of the knee should be initiated in the early stages of rehabilitation and progressed throughout the rehabilitation process until proper AROM heel/foot placement is achieve for optimal sprinting/running performance.
The initial stages of rehabilitation – During the initial stages of rehabilitation AROM exercises may be implemented at the same time the patient initiates their PROM exercises. In a standing position the patient will initially attempt to flex their knee to a 90 degree position or greater with the post-op knee pointed straight down toward the ground surface area (Figure 3a).
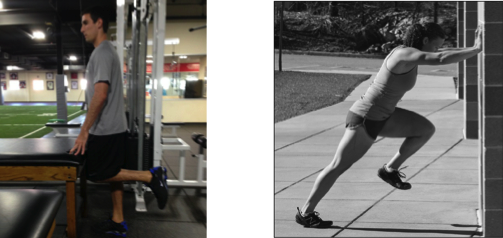
Figure 3a: Post-op Standing Knee Flexion, Figure 3b: Modified Wall Drill
Modified wall drills may also be incorporated when the patient/athlete is full weight bearing without the use of an assisted device. Wall drills are performed with the athlete facing a wall and placing both arms fully extended against the wall. The athlete assumes a slight forward lean in their posture and performs the exercise via the single post-op leg “stepping” or “marching” via hip and knee flexion and extension, as well as ankle dorsi flexion while maintaining this upper body posture throughout the exercise performance. Lower extremity exercise performance should occur with very little ground impact (Figure 3b).
The intermediate stages of rehabilitation – As the athlete progresses with their rehabilitation modified Mach drills may be incorporated, when appropriate, into the athletes program to continue to achieve the proper heel/foot and thigh height position necessary for optimal swing phase running performance. Mach drills are track and field drills established by track and field coach Gerard Mach that include the “A”, “B” and “C” series. Modified “A” marches may be instituted to also initiate linear movement during the exercise performance (Figure 4). Ground contact impact forces should also be kept to a minimum during the athletes exercise performance.

Figure 4: “A” Marches
The proper hip/thigh/knee height position during running performance is not also necessary for optimal running proficiency but also for the ideal application of force into the ground surface area. Often times the hip flexors are strengthened with the application of weight intensity during exercise performance. Although weighted exercise performance will increase this muscle group’s level of strength, often times the emphasis of the exercise performance is on the amount of weight the athlete can lift and not the appropriate height of the hip/thigh/knee during the exercise performance. Optimal hip/thigh/knee height also results in a favorable hip extensor range of motion (ROM) for ideal application of ground force production. This is analogous to the baseball pitcher who achieves a greater shoulder external rotation (ER) resulting in a greater ball velocity.
As the athlete progresses in their rehabilitation and exercise advancement is safely permitted, low impact butt kicks may now be performed at low exercise volumes. Butt kicks are performed with the upper body assuming the same position as wall drill performance. The difference with this exercise performance is as the athlete stands in place, both knees pointing toward the ground surface area. The athlete then “butt kicks” by alternatingly flexing each knee quickly while attempt to make contact with the heel of each foot at the corresponding gluteal fold (Figure 5).

Figure 5: Alternating Leg Butt Kicks
Mach “A” drills may also be progressed to “A” skips as the athlete now “skips” instead of marching emphasizing exercise technique with appropriate thigh height and heel position with corresponding low ground impact. The exercise is initially performed for short distances.
The advanced stage of rehabilitation – As the rehabilitation prescription progresses and the standing butt kick exercise is advanced to “continuous” butt kicks. The exercise is performed with the heel of each foot alternating rapidly to make contact with the buttocks for initial short durations of time.
“A” skips may be replaced with “A” runs. “A” runs are the last exercise instituted prior to the athlete’s initiation to actual running. “A” runs are performed with the athlete performing the “A” skip technique at higher velocities with a modified cyclical pattern, while attempting to have the heels of each foot make contact with each buttock. The rehabilitation professional should be aware that ground contact impact will increase due to the enhanced velocity of this exercise performance, thus the exercise should initially be performed for short distances and distances should be increased safely and appropriately.
Proper foot positioning is essential for backside and overall running mechanics. This foot placement is often overlooked during the rehabilitation process as emphasis is often placed of the achievement of full passive knee range of motion and not the active motion necessary for optimal running mechanics. Running is a cyclical event in nature and the ability to perform optimally during the swing phase will affect the efficiency and force output that occurs during the initial ground contact and stance phase of the sprinting/running cycle.




Nitpicking here, but I don’t think that is the best image used to show ideal recovery, as it seems like Bolt is slowing down in that stride. If you check some other races in slow-mo, he has a much better recovery phase. Not quite as clean as Michael Johnsons, but guess he really doesn’t need it to be perfect to be fast. And it is apples to oranges comparing a collegiate 5/8k stride to a world class 100m stride, totally different demands.
At 1:40 he lets off the gas and you see that similar recovery from your image.
https://www.youtube.com/watch?v=PH-3cHxXAK0
Brian,
Thanks for your post and the video. The purpose of the picture was to simply provide the reader with an illustration of the approximate proper positioning of the heel/foot.
Best,
Rob Panariello
Great article and Bob is a fantastic lecturer! If you ever have the chance to learn from him, take the opportunity.
Tony,
Thank you for the kind words.
Best,
Rob Panariello
I can speak from personal experience… there’s nothing worse than losing ROM after surgery. It feels awful. I wish every practitioner was aware of the signs so that swift action can be taken if the patient isn’t getting their ROM back. Let it go too long and it gets harder to return to symmetry. Striving for symmetric extension/hyperextension during an active heel lift is my top priority after surgery.
Sandy,
Keep working on that knee extension as THAT IS the top priority for knee ROM after surgery. Best of luck to you.
Rob Panariello
Nice article, good info!
Are u sure that figure 2 shows a female runner in a sprint event? Surface and shoes dont hint to that.
Ahh, seeing that Brian Dobens commented that as well, maybe you could use another picture? For example of a youth sprinter who lacks this technical feature? Otherwise the lady in figure 2 is just doing fine – because she simply doesnt sprint. 🙂
Chris,
I do appreciate both your and Brian’s comments. This article was written for the rehab specialist who would be working with athletes during the rehab processs. The illustrations that were selected were simply to correspond with the foot positions commented in the article. Certainly Bolt does not sprint with his arm position demonstated in the article, the female is likely not a sprinter, etc…
Best,
Rob Panariello