
Today, I’ve got a cool case study for y’all. It comes from guest contributor Travis Pollen – a very astute up-and-comer in the field of strength & conditioning. Travis’s results closely mirror the results that I achieved when I tested myself five years ago with bodyweight bridging variations when collecting data for my glute eBook. However, Travis’s case study is quite unique in that he has a prosthetic limb on his left side, which made for a very interesting analysis. I hope you enjoy the article!
Which Glute Bridge is Best?: an Amputee Case Study
by Travis Pollen
It’s well known that the supine hip extension, commonly referred to as glute bridging, is a phenomenal exercise for strengthening the glutes. But with so many variations to choose from using bodyweight alone – feet and shoulders flat on the ground, feet elevated on a bench, shoulders elevated (AKA hip thrusts), unilateral, bilateral, isometric, and dynamic – I’ve long wondered which is best for building the glutes. Due to the complex interplay of moment arm length, muscle length-tension relationship, range of motion, and stability demands of each version of the exercise, I turned to electromyography (EMG) to help answer my question.
What is EMG, Anyway?
Surface EMG is a measure of the electrical activity of a muscle, as determined by an electrode secured to the skin directly over the belly of the muscle. Generally speaking, the higher the electrical signal, the harder the muscle is working. There are a few caveats to this rule, but for our purposes it’s a decent assumption.
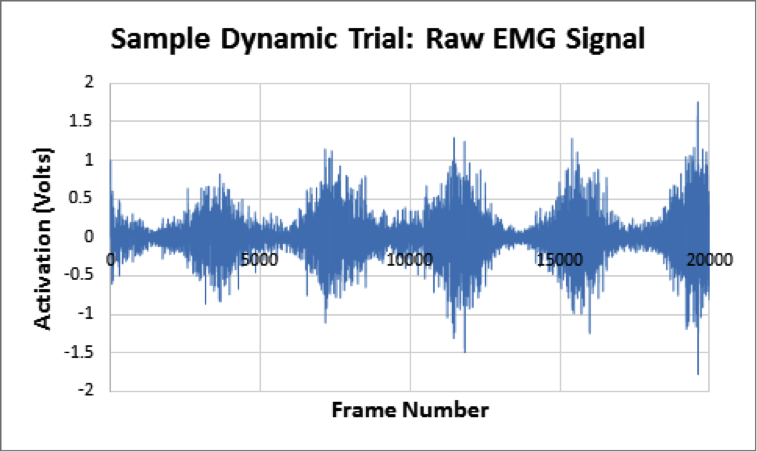
Unprocessed, or raw, EMG signal (pictured below) is expressed in volts, which isn’t a particularly useful metric. To interpret the data, we must first determine the maximum activation that a muscle is capable of producing. This maximum voluntary isometric contraction (MVIC) is performed as a brief, all-out exertion (against either a fixed object or manual resistance) in the position that allows for the target muscle’s optimal force production.
We then normalize (a fancy way of saying “divide”) all data from subsequent trials by the voltage obtained during the MVIC, which results in percentages of MVIC (% MVIC). According to the scientific literature, exercises with mean muscle activations of 60% MVIC or more are typically considered suitable for strengthening.
Amputee Case Study
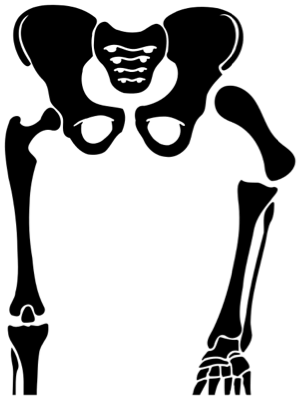
The present case study was performed on yours truly. I figured I’d make for an interesting test subject since I was born with proximal femoral focal deficiency (illustrated below), a rare congenital abnormality that resulted in the absence of my left femur and much of the accompanying musculature. (Fear not, though: my left glute is intact!). Thus, with my two sides alone, which I’ll refer to as “natural” and “prosthetic,” I can provide insights into both typical and altered muscle recruitment patterns.
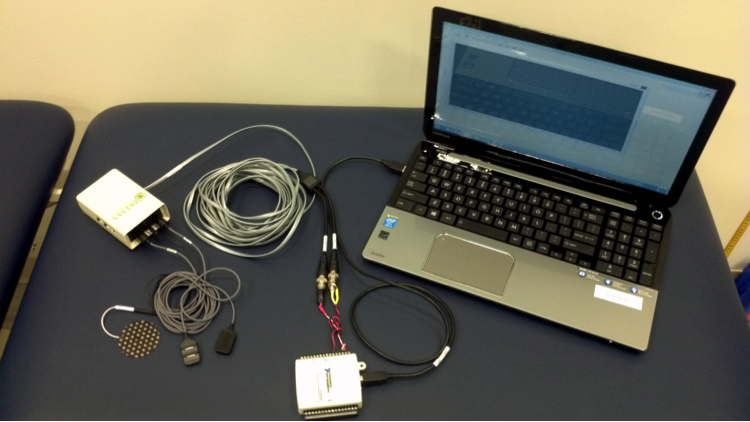
To perform the study, I used a Delsys Bagnoli 2-channel handheld EMG system consisting of two parallel bar surface electrodes (pictured below). After shaving and abrading the skin (special thanks to my girlfriend), I placed one sensor on each glute max parallel to the muscle fibers and halfway between the sacrum and the respective greater trochanters. I affixed the reference (ground) electrode to my ankle.
For the MVIC’s, I performed a manually resisted isometric quadruped hip extension (AKA donkey kick) on each side, collecting at a rate of 1000 samples per second. Next, I recorded five-second isometric holds for nine different bridging variations: three feet/shoulder positions (flat, feet-elevated, and shoulder-elevated) together with three leg positions (bilateral, natural side only, and prosthetic side only). Six of them are pictured below.

I also recorded 20-second trials of dynamic contractions (i.e. reps) for all the same exercises, utilizing a 2/0/2 tempo (two seconds up, two seconds down). The short trial durations were chosen to minimize the effects of fatigue, which is known to cause an increase in muscle activation. In addition, the order in which the exercises were performed was randomized with the same goal in mind.
Data Processing and Analysis (For the Techies)
As I alluded to earlier, a few things needed to be done to the raw EMG data in order to convert it to a useable format. This part gets a little technical, so be forewarned.
First, the data must be filtered to remove both high- and low-frequency content that isn’t physiologically based. Next, the data must be demeaned, meaning any overall offset from zero must be subtracted from each value. Then comes rectification, in which all the negative values are flipped to positives. A linear envelope is subsequently applied using a moving root-mean-square algorithm over 100-millisecond windows. Finally, the signals are normalized to the MVIC, resulting in the filtered EMG data used for analysis (pictured below).
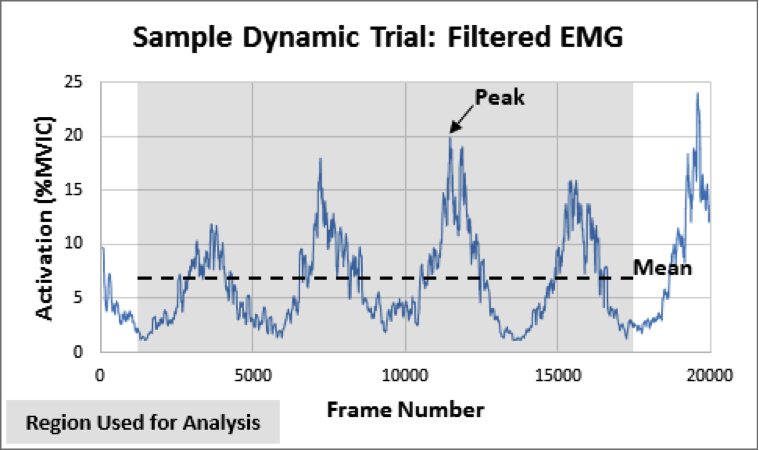
The metrics used for comparison of the various bridges were mean activation (the average activation over the entire trial) and peak activation (the maximum value obtained at any point during a trial). For the dynamic trials, only the middle four reps were included in the analysis.
And The Winner Is…
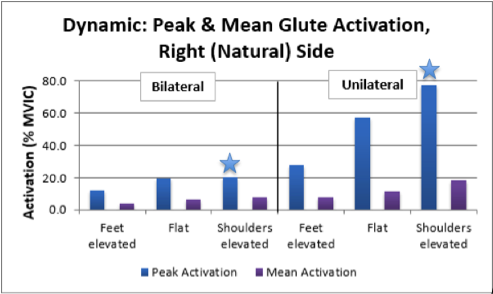
In general, the shoulder-elevated variations yielded the highest glute activation (in terms of both mean and peak), with flat bridging coming in a close second – especially on the prosthetic side – and feet-elevated bridging bringing up the rear, so to speak. The differences among feet and shoulder positions were greater for unilateral bridges than bilateral ones. The poor showing by the feet-elevated variations could be due to increased assistance from the hamstrings in that position.
On average, unilateral bridging elicited 2.3 times the activation (both mean and peak) of bilateral bridging for matched feet and shoulder positions, likely due to the additional stability demand in conjunction with the increased load. The greatest difference observed was between the unilateral and bilateral shoulder-elevated dynamic trials on the natural side (starred below), where the unilateral version had 3.8 times the activation of the bilateral counterpart. In short, the single leg hip thrust trumps the competition!
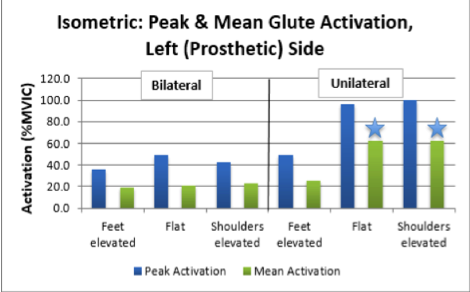
Across all trials, as percentages of MVIC the prosthetic side far exceeded the natural side. This means that the prosthetic side glute was working much closer to its maximum. Although the left versus right comparison tends to be muddied by precise electrode placement, the observed differences do make sense. My prosthetic side glute is much weaker than my natural one, so even bodyweight alone provides a big challenge. In fact, of all the variations tested, the only two that met the 60% MVIC mean activation threshold for strengthening were the prosthetic side unilateral flat and shoulder-elevated isometric holds (starred below).
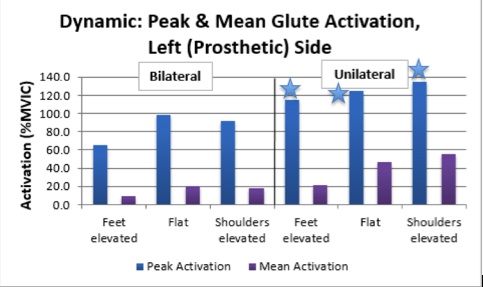
Interestingly, during all three unilateral dynamic trials on my prosthetic side (starred below), peak activation actually exceeded 100% of MVIC, with prosthetic side unilateral shoulder-elevated dynamic bridging (hip thrusts) coming in with a peak activation of a whopping 135%. Although these may seem like aberrant findings, it is not uncommon for muscles to activate to a greater extent during dynamic trials than during the MVIC.
Bottom Line on Bottom Training
Bodyweight glute bridging can provide a significant training stimulus to the glutes, especially for individuals with weaker glutes. To intensify the exercise, bridge with any or all of the following modifications:
1. Shoulders elevated (hip thrusts)
2. One leg at a time (unilateral), with the non-working limb tucked in towards the chest
3. Isometric hold in the extended position, by itself or immediately following a set of dynamic reps
4. Added external resistance in the form of a band, barbell, dumbbell, or chains
What’s Next?
In the future, I plan to expand this study to test more subjects and muscles (especially the hamstrings) as well as more hip extension exercise variations, including feet- and shoulder-elevated hip thrusts, which I hypothesize will elicit even greater activation than the shoulder-elevated version.
About the Author
Travis Pollen is an NPTI certified personal trainer and American record-holding Paralympic swimmer. He is currently pursuing his Master’s degree in Biomechanics and Movement Science at the University of Delaware. He has been featured on T-Nation.com, Schwarzenegger.com, MensHealth.com, and MOVE-Everywhere.com. He also blogs and posts videos of his “feats of strength” on his website, www.fitnesspollenator.com. Be sure to like him on Facebook at www.facebook.com/fitnesspollenator.






Cool study. However, you speculate that the glute of the prosthetic side has to work harder (% of MVIC) due to it being weaker – but couldn’t the higher percentage of MVIC of the prosthetic side cf. to the natural side also be due to the lack of any hamstring involvement in the movements on the prosthetic side, thereby making that glute making all the work?
Thanks, Kira! You raise a great point. In fact, that very explanation is something I was toying with, and it’s certainly plausible if we assume no hamstring involvement during the natural side quadruped hip extension MVIC. However, if the hamstrings were indeed assisting to some degree during the natural MVIC, then natural “maximal” glute activity may have been reduced, just like during the bridging trials. This would result in a level playing field in terms of natural and prosthetic percentages of MVIC, and my original explanation for prosthetic side weakness might hold true. All the more reason to repeat the whole thing with electrodes on the hamstrings to see what’s really going on!
Other than “rectification”, which sounds uncomfortable, this is just an excellent study. Thanks so much for sharing your work. Knowing the scientific background is invaluable to helping people get better.
Haha, thanks, Dunkman! Taking the lab science and actually applying it is really what it’s all about. That’s why I enjoy Bret’s work so much!
great article
Thanks, Justin! I really appreciate the kind words.
I do all of those variations and each one has its benefits however I always wondered which was the best for the glutes. I’m so glad you wrote this. Thanks for the great article!
Thanks, Diana! Sounds like you’re doing a great job of mixing it up.
This article is very interesting to me on a personal level because I am also an amputee and was born with PFFD. I have been trying desperately to find exercises I could do to work my glutes, squats seem to be out of the question as I just can’t squat deep enough with my knees at different heights. Balance can be an issue too. I have been doing straight legged deadlifts and using the seated leg press machine so far to work my glutes. I’ve tried hip thrusts/bridges in the past and sometimes they felt effective and other times felt like a waste of time. I’ll be keeping these findings in mind next time I attempt them and won’t discount them so easily. Thank you so much for this article. I’m still astonished I found it! LOL
Thank you so much for reading, Genevieve! We PFFDer’s have to stick together. It definitely took me a long time (and lots of help from my mentors) to figure out what to do in the gym to help — not exacerbate — my issues.
I have what sounds like a similar problem to you as far as bilateral squatting goes. My prosthetic foot doesn’t dorsiflex, so I end up going way up on the toes on that side, and I lose the proper forward tilt of my pelvis. One bilateral exercise I’ve had a lot of success with lately is the sumo rack pull (https://www.youtube.com/watch?v=FgS7KTrHhV0), especially when I really think about the mind-muscle connection with my left glute.
Two other things I recommend trying are glute bridging with hip adduction (stick a pair of sneakers between your knees) and hip abduction (with a mini-band around the knees). These variations help fire the glutes and anterior core in different ways, which may help recruit some of those weaker muscles.